
Transforming Rural Health Through Innovation and Evidence
Rural communities are navigating a difficult reality: Hospital closures, workforce shortages, and rising costs are colliding with increasing demand for care. At the same time, federal and state leaders are being asked to stabilize access, improve outcomes, and demonstrate responsible use of public funds, often within fragmented systems and tight resource constraints.
Through initiatives like the Rural Health Transformation Program, the Centers for Medicare & Medicaid Services (CMS) is helping states test new approaches to strengthen financing, expand access, and achieve better health outcomes. Turning these approaches into sustained impact requires aligning policy, operations, data, and delivery systems in ways that reflect the realities of rural care.
Organizations working in this space often need support translating new approaches into practice. Mathematica works alongside federal, state, and local partners from strategy and design through implementation and impact to strengthen rural health systems and make programs work better for rural communities.
Achieving Rural Health Transformation
CMS’s Rural Health Transformation Program (RHTP) offers the opportunity to redesign rural health systems at scale. Advancing rural health transformation requires coordinated support across policy, financing, analytics, and implementation—areas that must work together to produce measurable results for access and outcomes in underserved communities.
- For federal leaders: Success depends on the ability to optimize program operations, measure and improve performance, generate timely insights to guide decision making at scale.
- For states and providers: Implementing rural health transformation requires navigating complex program requirements, building partnerships, and developing solutions that reflect local needs while remaining evidence-based and moving forward.
Resources to Address Rising Costs
Rising healthcare costs make it critical for policymakers and program administrators to have clearer visibility into what’s driving spending growth and where interventions can have the greatest impact. Pricing and utilization data can help target reforms and track whether they improve access and reduce unnecessary spending.
Tools such as Mathematica’s Rural Health Potentially Avoidable Utilization (PAU) Dashboard give more than 1,600 rural hospitals nationwide insight into how PAU in emergency departments and inpatient settings impacts Medicare revenue—helping them identify where to invest to reduce potentially preventable, unplanned care.
We’ve also been a partner in developing resources such as a hospital cost tool and a health systems dashboard that provide policymakers and researchers with accessible data on hospital pricing, quality, and outcomes. These insights support federal and state leaders in making more informed decisions about where to invest and how to improve the efficiency of rural health systems.
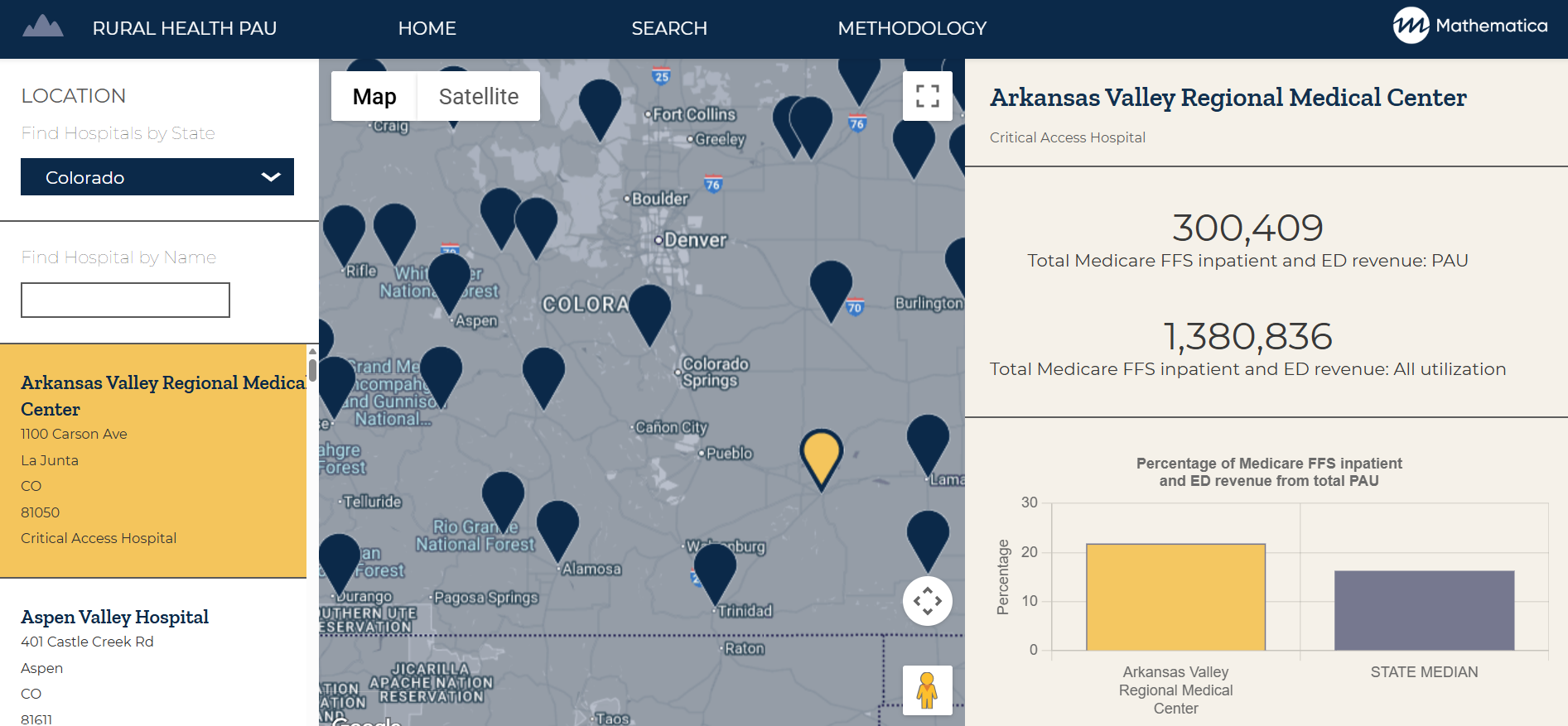
View Rural Hospital Data
Access potentially avoidable utilization rates by state for more than 1,600 rural hospitals using Mathematica’s updated interactive dashboard.
View DashboardTurning Data into Action in Rural Health Systems
Rural healthcare leaders face growing pressure to preserve access to care, improve outcomes, and maintain financial stability. As states implement rural health transformation plans, they need robust data and action-ready insights to understand what works, why it works, and how to scale it.
Mathematica's integrated analytics platform and advisory services help states and healthcare leaders make informed decisions rooted in evidence and local needs and meet key goals of the Rural Health Transformation Program.

Drive Sustainable Access and Innovative Care
Our analytics, policy, and program expertise combined with our technical assistance help states maximize federal funding and support care transformation efforts.
Learn MoreBuilding Capacity Under Real-World Constraints
Implementing rural health transformation requires coordination across agencies, providers, and community partners, often under tight resource constraints and evolving federal requirements. Building local capacity is critical to sustaining rural health transformation efforts over time. Technical assistance and training can help states and providers design and implement programs, monitor and evaluate efforts, and drive performance and quality improvement. This includes supporting CMS and states in implementing and evaluating Section 1115 demonstrations, aligning payment and delivery system reforms, and generating action-ready evidence to inform policy decisions. For example:
- The Rural Emergency Hospital (REH) designation allows communities that can’t support a full-service hospital to maintain 24-hour emergency, observation, and outpatient services. Through the REH Technical Assistance Center, Mathematica provides advisory services, financial modeling, virtual learning opportunities, and educational resources to guide hospitals through the transition process.
- As part of the Medicaid and Children’s Health Insurance Program (CHIP) Learning Collaboratives initiative, Mathematica helps the Center for Medicaid and CHIP Services provide high-priority policy and operational technical assistance to states and use program data to promote high-performing state health coverage programs.
- Mathematica leads the Technical Assistance and Analytic Support Program for CMS’s Medicaid and CHIP Quality Measurement and Improvement Program, which includes support for a core set of health quality measures. We provide support to states to reliably report these measures and use them to inform decisions about policies, programs, and practices to improve care quality.

Delivering Technical Assistance
Mathematica helps states and providers gain the skills, support, and tools they need to strengthen their research, evaluation, and reporting.
Learn MoreImplementing Alternative Payment Models
To curb rising costs and sustain rural healthcare, CMS and other payers are testing new approaches that reward care coordination, preventive care, and community health partnerships. These alternative payment models—including hospital global budgets—aim to stabilize financing while improving services for rural residents.
Designing and implementing these models requires coordination across payers, providers, and policymakers, along with strong financial modeling and data infrastructure to support decision making. In collaboration with the Rural Health Redesign Center and the CMS Innovation Center, our financial and data technical assistance is helping rural hospitals in Pennsylvania translate global budget models into practice.

Aligning Financial Incentives and Population Health
In Pennsylvania, global budget models helped hospitals cut Potentially Avoidable Utilization by focusing on better population health.
Learn MoreStrengthening Behavioral Health Services
Rural communities face unique challenges that heighten behavioral health needs—from provider shortages and geographic isolation to economic stress and limited access to broadband and transportation.
In many rural communities, improving behavioral health outcomes depends less on expanding a single service and more on coordinating care across primary care, social services, and community-based supports.
Mathematica works with the federal and state governments, health systems, and community organizations to strengthen behavioral healthcare by identifying gaps in services, evaluating what works, and translating evidence into practical strategies for states and providers.
We analyzed a large health system in the Dakotas and rural Minnesota that integrated behavioral health into primary care—leading to improved quality-of-care processes and reduced emergency department use. We’ve also studied programs that support parents with substance use challenges who are involved in the child welfare system, helping identify strategies to promote recovery and family reunification. These insights guide the development of scalable, evidence-based solutions tailored to rural realities.

Working with Iowans to Strengthen Community-Based Services
We’re helping Iowa improve community-based services for Medicaid beneficiaries with health, disability, and aging needs.
Learn MorePartners in Progress
We’re here to help states implement rural health transformation plans. Speak with our team of policy, data, and technology experts today.



